Baby boom, burdened women: The demographic rise behind Nigeria’s maternal mortality

A petty trader striving to support her family. Credit: Anibe Idajili
By Anibe Idajili
In Kontagora, a town in Nigeria’s Niger State, the air in the new market swirls with the scent of roasted maize and the fresh tang of tomatoes. Surrounded by the bartering of vendors shouting prices, a woman in a faded blue hijab pauses at a stall she’s known since childhood. She leans close to the vendor, a friend who has watched her children grow, and lowers her voice to a whisper.
“I’m pregnant again,” she says.
It is a personal secret slipped between friends, but the ramifications are anything but. Nigeria, home to just 2.92% of the world’s population, accounts for well over a quarter of all global maternal deaths. The quiet admission of a 32-year-old mother of five is a brief glimpse of a demographic explosion that is outpacing the country’s health infrastructure at an alarming rate. A sixth pregnancy pushes an already exhausted body into dangerous territory, raising the risk of severe hemorrhage or obstructed labour, conditions that demand emergency care often unavailable in under-resourced settings.
A Health System on its Knees
Nigeria’s maternal-mortality crisis cannot be understood without first confronting its birth-rate explosion. In 2023, the average Nigerian mother delivered 4.8 children; in 2024 that number had nudged up to 5.01. The increase unfolds against a backdrop of slow contraceptive uptake as only 15% of women now use modern family-planning methods, barely up from twenty years ago.
Nigeria’s population surpasses 240 million, and the northern region bears the brunt of this demographic increase. Here, cultural norms value large families, and more than a third of married women have one or more co-wives. But the dearth of clinics, trained birth attendants, and reliable contraception leaves women with few alternatives. Modern contraceptive use (MCU) among youth (15–24) in Northern Nigeria was only 3.9%, compared to 12.6% in Southern Nigeria between 2011 and 2021. In Niger state, women give birth to an average of 5.8 children, the highest of the seven states that make up the country’s north-central geopolitical zone. The implication is that each additional child adds a new demand on a health system already crippled by under-investment and a brain-drain of skilled staff.
Even in urban areas, the story is no less distressing. The average fertility in cities stands at 4.5, lower than the national figure of 5.3, but population density turns every fraction of a birth into tens of thousands of newborns each year. Hospitals scramble for beds, midwives juggle back-to-back deliveries, and emergency obstetric care becomes even more difficult.
Across Nigeria, women are forced to negotiate impossible choices. In Rigolo, a remote Niger State village, a woman in labour must travel many hours by road to Yauri General Hospital in neighbouring Kebbi State for a caesarean section. Meanwhile, in Lagos, a full-time petty trader cannot afford the transport costs for the four antenatal visits doctors recommend. These everyday hardships explain why Nigeria’s maternal mortality ratio remains high at 1,047 deaths per 100,000 live births. The baby boom strains an already fragile health system, turning avoidable deaths into a national crisis and pulling the country farther from the Sustainable Development Goal Target 3.1, which aims for fewer than 70 maternal deaths per 100,000 by 2030.
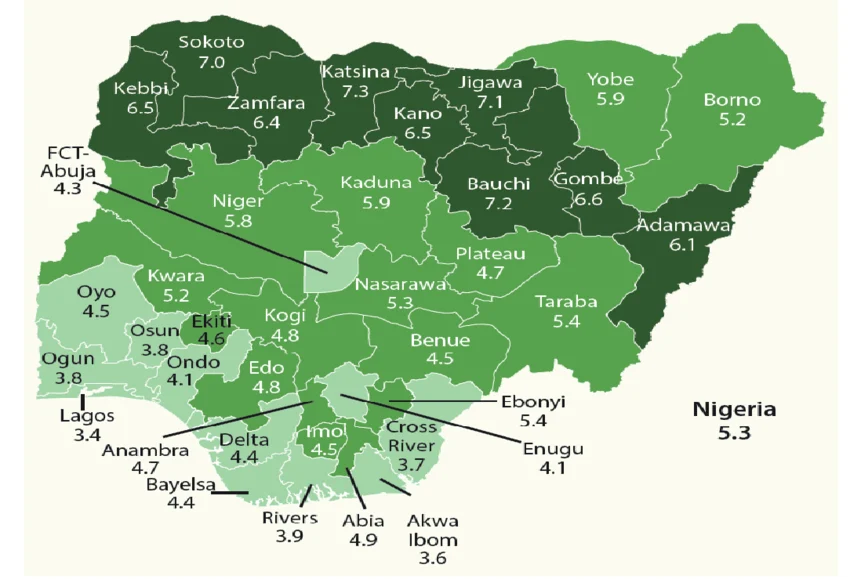
Total fertility rate by state. Credit: Okafor Samuel
The Strain on Hospitals and Clinics
Scrutinizing the Federal Ministry of Health and Social Welfare’s budget reveals a mismatch between Nigeria’s maternal-health pledges and its fiscal actions. In the 2025 budget, allocations for family planning, a key component of maternal health, were slashed by 97%, falling from ₦2.225 billion in 2024 to ₦66.39 million. This cut has raised concerns about Nigeria’s ability to achieve its FP2030 targets. Adding to the concern, as of last month, the Minister of Health, Prof. Muhammad Ali Pate, reported that only ₦36 million of the ₦218 billion capital health budget for 2025 had been released, signalling implementation challenges for the promised maternal-health interventions.
The consequences are visible inside Rigolo Primary Health Centre (PHC), where a midwife gestures to a row of empty shelves. “We lack the drugs to stop bleeding after delivery,” she says, holding up a half-filled ampoule of oxytocin. “When a woman arrives in hemorrhagic shock, we can’t intervene fast enough because the medication is not available.” The result is a rising number of home births, often assisted by traditional birth attendants (TBAs) or untrained relatives, leaving complications untreated and causing a rise in maternal mortality.
The Prenatal Care Gap
The lack of antenatal visits in certain parts of Nigeria is a missed opportunity to catch and treat conditions before they become serious. The 2021 Nigeria Multiple Indicator Cluster Survey (MICS) reports only 30.50 % of women in Sokoto State (North) attended antenatal care and saw a skilled health personnel at least once, contrasted with 96.8% in Imo State (South). Urban centres report a healthier 74.3 % delivery rate in facilities, while rural areas lag at 34.5 %.
Midwives in Lagos, Kano, and rural Ebonyi tell a similar story. “We try to reach out to women in the community, but the distance between villages and the nearest health post can be 40 kilometers,” says Chioma Eke, a community health worker in Ebonyi. “If a woman has to walk for three days to get to a clinic, she will only go when the baby is already overdue, or the mother is already in trouble.”
Such delays translate directly into mortality. A Demographic and Health Surveys (DHS) analysis confirm that fewer than the recommended number of antenatal care (ANC) visits raise the risk of pregnancy-related complications and mortality, especially in poor communities plagued with transport gaps, out-of-pocket costs, and cultural restrictions.

When the Law Pushes Women into Danger
Nigeria’s penal code permits abortion only when a woman’s life is at risk. The country’s high fertility rate and limited access to contraception, however, has created a hidden market for termination services. Interviews with women who have sought clandestine abortions reveal a network of “MTP” clinics that operate in repurposed shops and even private homes. These clinics are unregulated, often run by individuals with minimal medical training, and rely on nonprescription medicines, herbal concoctions, and dangerous surgical procedures.
One woman, who asked to remain anonymous for fear of reprisals, described her experience: “I was 19 and pregnant with my second child. My family could not afford another baby. I went to a ‘clinic’ in a rural community in Adamawa State. The person gave me pills, told me to lie down, and left. Two days later, I was bleeding heavily, and I had to be taken to the hospital with a ruptured uterus.” She survived but bears a permanent scar and a distrust of the health system.
Ernest Orji, Professor of Obstetrics and Gynaecology at Obafemi Awolowo University, Ile-Ife, Osun State, has linked about 40 % of maternal deaths in Nigeria to complications from unsafe abortions. Chemist/Pharmacy units were responsible in 51% of the abortions, whereas abortions performed in Clinics stood at 29.4% of cases. On a global scale, about 5 million women are hospitalized each year for treatment of abortion-related complications such as hemorrhage and sepsis, and abortion-related deaths leave 220,000 children motherless.
When legislation forces women into unregulated care, the true victims are the mothers whose lives are shattered in the process.
Nigeria’s Maternal-Health Fight
Janet Adonai Muazu, a retired nurse and midwife in Niger State, recalls a night in the delivery ward of a PHC when two women arrived, each showing signs of postpartum hemorrhage. “We only had one blood pressure cuff and one set of sterile gloves,” she says. “We had to improvise, sharing equipment while trying to keep each woman alive.
In Kontagora’s Tundun-Wada Maternal & Child Health Centre, women delay seeking care because of fear of stigma or cost. “Many of them come after five or six months of pregnancy, already exhausted, and we cannot guarantee a safe delivery,” Bernice Egboche, the Nurse-in-Charge, explains. “We have to prioritize those in critical condition, and the rest leave with a promise to return, often a promise they cannot keep.”
In Eneji community of Kogi State, community health worker Bala speaks of a different challenge: cultural resistance to family planning. “Many elders believe that a woman’s worth is measured by how many children she bears,” he says. “When I try to give out contraceptives, it feels like I’m fighting a battle against tradition.”
Despite these challenges, pockets of progress are emerging. In Kano State, Nigeria, initiatives like the Smiles for Mothers program introduced heat-stable carbetocin (HSC) to more than 87 health facilities to improve postpartum hemorrhage (PPH) prevention. This addresses challenges with cold-chain storage for conventional oxytocin, aiming to reduce high maternal mortality rates. Lagos state also actively adopts HSC alongside oxytocin and misoprostol to prevent maternal deaths.
These drugs retain potency even in Nigeria’s hot climate, directly addressing the high PPH rates that have long plagued maternal health outcomes. While the reach is still limited, the combination of political will, practical drug choices, and community engagement can improve maternal health.

What Realistic Reform Would Look Like
Nigeria’s population is on track to exceed 360 million by 2050, and this puts unprecedented pressure on a maternal health system already stretched thin. What, then, does a realistic, evidence-based reform look like?
First, according to Ken Nnaji, a maternal health advocate, the government must close the gap between family-planning budget allocations and actual disbursements. “An independent oversight board, comprising civil-society representatives, health experts, and members of the legislature, could audit procurement processes quarterly, ensuring that funds earmarked for contraceptives reach the intended facilities.”
Nnaji also advocates for a health-system strengthening that prioritizes the scaling up of skilled birth attendants. “Our work in rural communities has shown that an increase in trained and skilled birth attendants can prevent thousands of deaths annually. But the issue is that training alone is insufficient because health workers need housing subsidies, hazard pay, and career-path incentives to stay in underserved rural areas.”
He adds that community engagement is also very important. “We work with religious and traditional leaders to shift cultural beliefs around family size and create an environment where women feel empowered to use contraceptives. We have supported community-led dialogues to increase contraceptive uptake.”
Legal reform also plays an important role. Lawyer John Itodo argues that, “expanding lawful abortion grounds, including fetal anomaly, rape, and socioeconomic hardship, would curtail unsafe “MTP” clinics and result in a decline in abortion-related related maternal mortality.”
Studies have also found that digital technology can bridge the distance between women and health care. Mobile health platforms can send SMS reminders for antenatal appointments, provide tele-consultations, and deliver information on danger signs. Scaling these solutions, with the support of telecom regulators and private partners, could improve early detection of complications.
A coordinated strategy involving fiscal accountability, workforce incentives, community engagement, legal reform, and digital innovation offers a practical pathway to protect millions of Nigerian mothers. Acting now will save lives and secure the health of a country poised for unprecedented growth.